Community members grab sanitary products from NYC Health during a Monkeypox outreach event. Churchill Ndonwie for the Bronx Inc.
Bronx community leaders gathered for a night of Monkeypox outreach Wednesday, to raise awareness about the spread of Monkeypox in the Bronx and address the disproportionate impact the disease has on Black and Latino communities.
Members of the community were given information about vaccination resources and educational pamphlets on how to protect themselves from Monkeypox. They were also given condoms, sanitary products and encouraged to seek care if they feel sick or identify a rash or sore.
“We know that inequities continue to exist. The numbers within our communities, particularly communities of color among African American and Latino men are still high when compared to other groups” said Bronx Borough President Vanessa L. Gibson, who’s office hosted the event in partnership with the Bronx Chamber of Commerce, Third Avenue Business Improvement District, NYC Health and Destination Tomorrow.
Though cases are beginning to decline citywide, latest data from New York Health as of September 18 shows 632 of the identified 3480 citywide cases are in the Bronx. And of those citywide cases, 60% are among Blacks and Hispanics, the majority demographic group of the Bronx.
“Lot of people out there haven’t been able to get the education that they desperately need in order to understand and take the steps that are necessary to protect and prevent from being harmed by it” said Sage Rivera, Chief Development Program Officer for Destination Tomorrow, a grassroots agency and the LGBTQ+ center for the Bronx borough. The center also serves as a first dose Monkeypox vaccination site.
Rivera also talked about the importance of not falling prey to stigmatization against a certain community because they are the most affected. “It’s very, very easy to fall into the trap of what’s going on, because it’s been so prevalent amongst people of color, and affecting so much the LGBTQ community. This is a skin to skin contact disease, plain and simple,” he said.
On July 18, the five Borough Presidents sent a joint letter to the Centers For Disease Control and Prevention Director Dr. Rochelle Walensky demanding more Monkeypox vaccines be sent to New York City. Latest New York Health data shows 95,345 doses have been administered citywide with 5,639 doses administered in the Bronx. About a third of the citywide doses were administered to those identifying as Black or Hispanic.
“We do know that access is an issue. So we want to get more vaccination sites,” said Anita Reyes, Assistant Commissioner, Bronx Neighborhood Health, Department of Health and Mental Hygiene.
New York City Health recently opened a Tremont Monkeypox vaccination clinic in the Bronx. The clinic, located at 1826 Arthur Ave., is open to the public for first dose vaccination walk-ins.
“I think that health is an issue that is still not spoken about enough in the Bronx….Monkeypox is just something that is making a lot of people question what makes them feel safe and healthy in a community, especially for the LGBTQ community,” said Cecil Brooks, a long time Mott Haven resident.
“If we have enough people who are fighting misinformation, and know what resources are available, then we can do our small part to make the South Bronx an even better and more welcoming space,” Brooks said.
The tiny waiting room of Dr. Andrea Littleton’s Bronx office was overflowing by the time she arrived in the late morning. Some patients sat in stony determination while others paced impatiently in the hallway — clawed by addiction and anxious for the relief that Littleton could provide. One dozed, slouched in his chair beside the inner door that leads to the claustrophobic medical office where, twice a week, Littleton prescribes buprenorphine to opioid addicted patients.
Littleton has worked for 15 years at Care For The Homeless, a non-profit medical center that provides medicine-assisted treatment for the homeless who suffer from opioid addiction. Medicine-assisted treatment is considered the “gold standard” for opioid use disorder, and the medications used are typically either methadone or buprenorphine (also known as Suboxone).
Littleton’s office, situated in Hunts Point in the Bronx, is at perhaps the very heart of New York’s opioid epidemic. In 2018, the overdose deaths per capita in Hunts Point was over 2.5 times the city-wide average, according to a 2019 report from the Department of Health and Mental Hygiene.
Only Staten Island ranks above the Bronx in terms of number of opioid deaths per capita. However, treatment in the two boroughs looks very different.
“Even though both [Staten Island and the Bronx] are epicenters of the opioid epidemic,” said Littleton. “There are far more [buprenorphine] prescriptions being written in Staten Island, but not necessarily more providers.”
A 2018 research report confirms Littleton’s observation: patients in Staten Island receive buprenorphine 3.6 times more frequently than those in the Bronx. Patients in the Bronx are, likewise, 3.2 times more likely to receive methadone. All this while the Bronx has nearly three times as many physicians who are able to prescribe buprenorphine, according to federal data.
“[Buprenorphine] certainly offers more freedom and flexibility,” said Littleton. Some patients refer to methadone treatment as “liquid nails,” she said. “They can’t go anywhere else or have a job or travel even because they have to be there every day.”
Having to show up at the clinic every day to receive treatment is not only a burden on methadone patients. The clinic itself can be stressful. “There is also a lot of stigma,” said Littletone. “People know where [the clinics] are, they don’t feel safe there. And it’s triggering because there might be someone selling right there in the waiting room or right outside the door.”
Finally, the medication itself makes a difference. Buprenorphine lacks some of the negative side-effects that methadone is notorious for. On Buprenorphine, patients “can go about their day feeling normal, they don’t feel high, they don’t feel loopy, they just feel normal,” Littleton added. “Where as a lot of people on methadone feel high, they can’t think clearly, they feel like they can’t maintain their normal activities.”
In 2018, Canadian researchers published guidelines recommending buprenorphine as the preferred first-line treatment for opioid addiction, only switching to methadone for patients who respond poorly to buprenorphine or who express a strong preference.
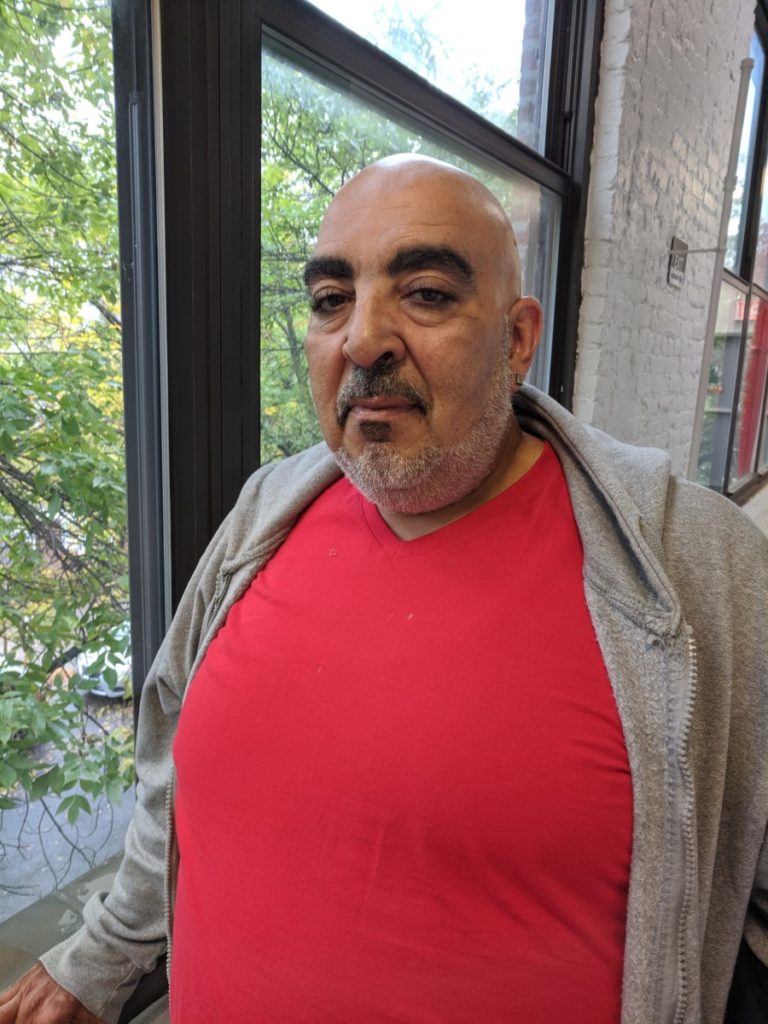
Salvador, who asked that his last name not be used, is a big man with tired eyes and a tidy grey beard. He is one of those patients who depends on the buprenorphine he gets from Littleton every week.
“When I have these,” he said holding a zip-lock bag containing week’s supply of individually-packaged pills, “I don’t even think about [heroin]. But without them, I have to use.”
But that reliance on Littleton can spell disaster if she is not available.
Salvador had been clean for nearly two months, he said. But, when Littleton had been away the prior week, he hadn’t been able to find another prescriber. Salvador had gone back to heroin to satisfy his cravings.
Salvador had been clean for nearly two months.
“You abandoned me,” Salvador sulked jokingly. But the damage done is no laughing matter.
Now, Salvador will have to endure the unpleasant, and potentially dangerous, process of reinitiating his treatment. Buprenorphine includes naloxone (the active drug in Narcan) which can precipitate withdrawl if patients start treatment too soon after using. Complications from withdrawl, including dizziness and asphyxiation can be severe. He will have to start the first stages of withdrawl from the three baggies of heroin he snorted that morning before he can take his first pill.
Despite the success of buprenorphine, getting access to treatment still remains a problem for many Bronx residents. In February 2019, the New York State Department of Health released new guidelines encouraging SAMHSA-approved doctors to “start prescribing buprenorphine, and if already prescribing to increase the number of patients under care.”
But the question remains, why do these two boroughs, facing the same crisis receive such different modalities of treatment?
From the start, buprenorphine treatment catered to affluent white patients who did not want to be associated with the stigma of receiving treatment at methadone clinics.
“In the case of opioids,” writes Dr. Helena Hansen, Associate Professor of Psychiatry at NYU Langone. “Addiction treatment itself is being selectively pharmaceuticalized in ways that preserve a protected space for White opioid users.”
Buprenorphine was developed in 1966, but failed at catch on until it’s resurgence 30 years later, which, argues Hansen, coincides with the rise of opioid use in white communities. When buprenorphine was legalized as a treatment for opioid addiction, in the 2000 Drug Addiction Treatment Act (DATA 2000), a group of lawmakers who opposed the DATA 2000 bill foresaw that it would “consign ‘hard core’ users to the existing and widely recognized as failed system.”
Sure enough, as the opioid epidemic exploded in in New York City, buprenorphine was increasingly available only to those who could afford private insurance. Between 2009 and 2016, the number of buprenorphine prescriptions on private insurance increased by over 4.5 times, while the number on medicaid fell nearly by half. In 2016, over three-quarters of buprenorphine prescriptions were paid for by private insurance.
While the city’s $60 million HealingNYC initiative has shown modest success in reducing the number of overdoses city-wide and increasing buprenorphine prescriptions, it hasn’t been enough in the Bronx, where opioid deaths continue to increase.
“It’s supply and demand,” said Dr. Tiffany Lu, Medical Director of the Montefiore Buprenorphine Treatment Network. “The Bronx does not have enough capacity because it historically had the burden of the disease.”
And while money for outreach and education programs are essential, the greatest hurdle in the Bronx is finding physicians like Littleton and Lu who are able and willing to prescribe buprenorphine.
Under DATA 2000, prescribers are required to obtain special wavers to even be allowed to prescribe the treatment.Completing the requirements can be an arduous burden to already-overextended care providers. Doctors are required to attend eight hours of training and clinicians (including nurse practitioners and physicians assistants) are required to take 24 hours of training.
However, once a physician has a waiver to prescribe buprenorphine, they are only allowed to treat 30 patients in their first year. This cap increases to 100 and 275 patients in their second and third year, but the cap still contributes to the shortage of access to buprenorphine prescribers, according to a letter by the New York State Department of Health.
Some physicians question the need for a waiver at all. “[Buprenorphine is] a schedule III drug,” said Littleton. “It’s less addicting substance than opiates, but prescribers are able to provide [opiates] at will without training.”
A bipartisan bill, the Mainstreaming Addiction Treatment Act of 2019, has been introduced to both the House and Senate. The bill would allow physicians to prescribe buprenorphine without a DEA waiver.
Still, even some physicians who interact with opioid-addicted patients may be reticent to start buprenorphine treatment.
Rikin Shah, Chief Resident at St. Barnabas Hospital in the Bronx, is not waivered to prescribe buprenorphine. In the emergency department, where he typically encounters such patients, initiating buprenorphine treatment would require counseling and monitoring, and in a 200-bed room, where other patients require attention, he doesn’t feel that starting new medication is a good idea.
“We may not be able to monitor how they are doing on the medication, whether they need changes in doses, or if they are having any adverse drug/side effects,” Shah wrote in an email. “This is dangerous for our patients.”
Emergency departments are not the appropriate venue for starting addiction treatment, Shah continued, and promoting them as such might lead to an abuse of their resources.
“We need to optimize our resources to taking care of the sickest patients and to those who are at risk of losing their life…. More often than not, although withdrawal symptoms are uncomfortable, they are not life threatening,” Shah’s email continued. “Emergency departments become in a way suboxone/methadone clinics as patients can find coming to the [emergency department] the most convenient way to treat their withdrawals.”
While some physicians may be reticent to provide treatment for medical reasons, their own stigma towards addiction may be just as big a barrier.
Littleton in her Bronx office.
“Lack of knowledge and fear of the unknown are big factors, and the other is stigma,” said Littleton. “People get concerned about [treating] the patient who has an addiction and what that means.”
Some providers worry that treating addiction is like “opening up a Pandora’s Box,” said Littleton. They think “if we talk about [your addiction] we’re going to talk about all that trauma that you had as a child and I don’t have the resources to give you the support to deal with that, I don’t have access to good mental health [services] that I can connect you with… and I can only address so many things in 15 minutes.”
Littleton walks through these traumas with almost every patient she sees. Raymond, who had recently been released from Rikers on drug charges and asked that his last name not be used, told Littleton that he’d been using speedballs (a mixture of heroin and cocaine) since age 11, when his father introduced him to the dangerous cocktail.
Littleton didn’t blink when Raymond said that he’d had a relapse. Like Salvador, he relied on heroin to tide himself over after leaving prison, before coming for treatment. Instead of discharging patients who relapse, punishing “dirty urine” by terminating treatment, Littleton stresses the importance of patience and understanding.
“Many [patients] will have a relapse, and that’s okay,” she said after seeing Raymond out. “Addiction is a spectrum… [and] we do them a disservice by discharging them.”
Once physicians can normalize their understanding of addiction, and see the effect of treatment, those fears and stigmas will fade, Littleton said. “It’s just understanding that… anybody can have opioid use disorder and have perfectly normal lives otherwise.”
Treating opioid addiction is no simple task, and buprenorphine is not a silver bullet, said Lu, the doctor from Montefiore. But, access and supply are the only way to get this life-saving drug into more hands.
“[Being trained to prescribe] buprenorphine is the lowest threshold that anyone can do.” Lu said. “My message to all my colleagues is: please do something, get yourself trained, offer it, because if you don’t offer it you’re basically saying you’re not interested in treating the disease in any way.”
Community members lit candles Aug. 30 in memory of those who have died of heroin overdose in the Bronx.
MOTT HAVEN–Walking through the streets of the South Bronx one afternoon in July, Tino Fuentes, 53, said he sensed trouble across the street.
“You get this little gut feeling like something’s not right,” Fuentes said.
He found a man on the ground, unresponsive, drawing faint, shallow breaths. Bystanders said the man had been unconscious for several minutes, and his breathing was getting weaker as time passed. Amidst the chaos, a woman leaned over and whispered, “He did a bag.”
Fuentes, who knew she meant the man was likely overdosing on heroin, said he sprung into well-rehearsed action. An ambulance had already been called, but in the case of an overdose, every second matters. An injection of the drug Naloxone can reverse the effect of opioid overdose, but the success rate depends on rapid response.
Fuentes had a Naloxone kit across the street. After retrieving it, he removed the orange top of the vile, filled the syringe with its contents, and plunged the two-inch needle into the sinewy part of the man’s shoulder. Fuentes said he was rolling the man over to begin rescue breathing when he came to — brought back by the medication Fuentes injected.
“It’s such a selfish feeling, but I feel great. I just saved someone’s life,” Fuentes recalled.
Fuentes claims to have saved more than 75 lives with Naloxone since 2006, though he said he has lost count. He is not an EMT or doctor. He just makes sure he always has a kit on him when he is walking around New York.
“I do this because I came from these streets,” Fuentes said. “I gotta find a way to give back, you know?”
Fuentes serves as the co-director of the Syringe Exchange Program at St. Ann’s Corner of Harm Reduction in the South Bronx, where he also trains other people to administer Naloxone. Under New York State law, anyone can carry the medication after undergoing the twenty-minute training and earning a blanket-prescription.
“There is really no reason not to get trained,” Fuentes said. “We’re reaching out to try to train everybody.”
https://www.instagram.com/p/BJ3QDvmDpBV/
Between 2014 and 2015, Mott Haven and Hunts Point had the highest rate of heroin overdose in New York City by a significant margin. The death rates have steadily increased in recent years. Joyce Rivera, founder and executive director at St. Ann’s, said socioeconomic status and race cause people to ignore this public health crisis in the Bronx.
“The only people who really pay the price for using drugs are poor, working class people,” Rivera said to a crowd on National Overdose Awareness Day at the end of August. But she said harm reduction programs and Naloxone are saving lives in marginalized communities. “Every life matters. Who’s life is expendable?”
Across the country, heroin is becoming increasingly deadly. New reports confirm that heroin is now commonly cut with prescription Fentanyl, a drug 100 times stronger than morphine, causing users to underestimate the potency of what they inject.
“[Dealers] put whatever they put in heroin to stretch it out, to make more money,” Fuentes said. “Not too many people know what’s being put in there.”
According to Fuentes, the man he saved in July was a frequent user, injecting up to five bags a day. The day he nearly died, he was only on his first bag, which he had sniffed rather than injected. Since those are not the conditions that generally lead to overdose, Fuentes said he suspects Fentanyl was present in the mixture. Naloxone is still effective against Fentanyl-laced heroin though experts say in those cases it might take more than one dose to revive the person.
Since the Naloxone program began at St. Ann’s in 2006, awareness around heroin overdose has increased dramatically in New York. Now, all police officers in Mott Haven carry Naloxone. Overdose response trainings are being held in local prisons. Laws around prescription to carry have changed to give easier access to the life-saving medication.
Organizers at St. Ann’s say the shift in awareness and action was influenced by the changing demographics of heroin use and abuse throughout New York State. In 2013, more white New Yorkers than black or Hispanic New Yorkers died of overdose statewide.
“The progress we have made, the general tipping point we have passed, has to do with all of the white people who have overdosed,” said Bill Matthews, clinical director at St. Ann’s.
For Fuentes, it’s frustrating to believe nobody cares about the Bronx. But he said the most important thing is that progress is finally being made, and it’s helping people and saving lives.
The AIDS Walk participants march down Southern Boulevard raising awareness for HIV/AIDS in the South Bronx (BENJAMIN BERGMANN/The Bronx Ink)
Against the backdrop of gray skies, the roughly 100 participants of the Third Annual Community Board 2 AIDS Walk replaced the usual truck racket in the area with the odd chants of “HIV! GET TESTED!” and “SAFE SEX! USE CONDOMS!” Marching between Westchester and Hunts Point Avenue, the group called attention to the community-wide stigma of the disease, something the organizers believe may be a key obstacle to eradicating the virus. “We need to break the silence once and for all,” said Millie Colon, a community board activist and chairperson of the AIDS Walk. “People are no longer dying for lack of medication, but rather due to a lack of communication and education.” Silence is literally killing some Bronx residents. Colon encountered AIDS over 20 years ago when her nephew passed away from the disease. Three years ago she lost her brother to AIDS, after he spent four years refusing to see a doctor for fear of community backlash. Though the fight is deeply personal for her, Colon recognizes the larger context. She urged the community to overcome the “fear barrier” of getting tested, and she encouraged those who are infected to “come out of the closet” and receive the proper medication.
Millie Colon, chairperson of the Community Board 2 AIDS Walk, rallies the marchers before the walk begins in Hunts Point (BENJAMIN BERGMANN/The Bronx Ink)
From time to time the marchers, color coordinated in red and white, stopped along the 45-minute route to listen to community voices and pray for those that have lost their lives to a disease first recorded in the city 33 years ago. One of the marchers, Carmen Rodriguez, surprised many by revealing that her husband, who had been secretly living with HIV for 25 years, passed away last Monday. “He didn’t want nobody to know” she said, gently dabbing at her mascara-stained tears. “He was in denial for many years and when he started treatment eight years ago, it had already caused too much damage.”
Carmen Rodriguez stands outside the Hunts Point Recreational Center after revealing to the group of marchers that her husband passed away from AIDS just last week (BENJAMIN BERGMANN/The Bronx Ink)
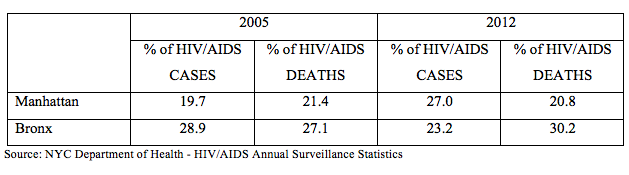
Rev. Kahli Mootoo, a Hunts Point pastor and former AIDS activist, commanded the megaphone for large parts of the walk, educating sidewalk spectators on the importance of getting tested. “The issue of HIV is losing steam” he said. “People are no longer scared of it, but does that mean they are not getting infected? Of course not!” Even though HIV numbers are consistently falling across the city according to the New York City Department of Health, the percentage of people dying from the disease continues to skew heavily towards low income neighborhoods. The Bronx has the highest death rates among the five boroughs, while Manhattan has the clearest survival advantage in New York City. These numbers were much more even back in 2005. Though the organizers did not focus on these issues, Rev. Mootoo himself believes the issue is deeply entangled with poverty and political will. His view is that as long as HIV-related issues are contained in the most disenfranchised neighborhoods, city officials will see no reason to take action. “We always say the squeaky wheel gets the oil. Our community doesn’t have the power to squeak loud enough,” Mootoo said with a smile. “And god knows we could use some more oil around here.”
Carmen Arias, an employee at Blended Up juice bar in Soundview, preparing pineapple smoothies to-go. (JENNIFER LUNA/BronxInk)
Bright orange carrots and yellow cubes of mango spun into liquid inside large plastic blenders one September afternoon at Blended Up, a new juice bar on Westchester and St. Lawrence Avenues in the Bronx. A steady stream of customers ordered smoothies named “big-fighter” or “detox power.” Many said they were grateful for a healthier option to the more established fast-food fare at the nearby Checkers, McDonalds and Dunkin’ Donuts, according to owner Maribel Vilas, 44, a native of Puerto Rico.
“There’s a misconception that black and brown people don’t want to eat healthy,” said Yasmin Tejeda, 28, drinking a mango smoothie on her lunch break from Primary Care Information Project where she is a clinical quality specialist. “But if it’s affordable and it’s available we want to eat it.”
Fresh juices are quickly becoming a staple in the local diet and economy. Vila’s business is the newest of four juice bars that have opened in the Soundview area of the Bronx within the last five years, three of them just within the last year.
The trend began in 2010 when Rapper David Styles—known by fans as Styles P—opened the popular Juices for Life on 1026 Castle Hill Ave. Its success inspired other Bronx entrepreneurs to follow suit. Three years later, Fresh Take, a juice shop on 2245 Westchester Ave., opened its doors and four months ago, GP Smoothies and Gift Shop opened on Castle Hill Avenue. Fresh Take owner Eric Glisson, 38, said the shop sells up to 400 juices a day, with many of the customers coming in after a work out at the Planet Fitness gym above the shop.
Dr. Samuel Walters recommends juicing to his patients, many of whom are diabetic or pre-diabetic. (JENNIFER LUNA/BronxInk)
“People were so excited and very receptive, saying, ‘Thank God something healthy is coming to the neighborhood,’” Glisson said. GP Smoothies and Gift Shop owner Geoconda Pin said she distinguishes her business from others by including a deli and groceries. Juices, however, are still her most popular product. “People like the concept of green juices,” Pin said. “We use vegetables and natural fruits and that’s why they buy a lot.”
Affordability is key to business in Soundview. A small juice at Blended Up and Fresh Take sells for $3.50, compared to $5 at Juices for Life. Some customers compare the cost favorably to fries and a shake at McDonalds. “You can’t be a juice place coming in here selling a ten-dollar organic juice,” said Nancy Guevara, 28,a Bronx native who was visiting from Pennsylvania.
Prices don’t seem to be a factor for many customers, especially when their doctors recommend the products. Dr. Samuel Walters, an Internal Medicine specialist in Unionport, estimates 20 percent of his patients to be diabetic and 70 percent hypertensive. Juicing, the doctor said, is a good way to get fresh fruit. “I am a naturalist in the way I treat patients,” the Jamaica born doctor said. “Patients ask if I recommend juice and I do.”
But his recommendation comes with a caveat. Diabetes rates are high in Bronx neighborhoods. According to the New York City Community Health Survey of 2002 to 2004, the greater Pelham Bay area had a diabetes rate of 11 percent. In 2010, the Center for Disease Control reported that 8 percent of Americans have the disease. Restricting calories, Dr. Walters said, is the key to losing weight and keeping diabetes in check.
An improved diet and increased exercise also helps. Orlando Castro of Soundview dropped 50 pounds over the last year by making these lifestyle changes. The 31-year-old lives near Blended Up and comes for breakfast frequently throughout the week. “My father died of diabetes and my mother has diabetes,” Castro said, sipping on a strawberry and pineapple smoothie. “I’m not going out that way.” Some health experts, however, are concerned about the dangers of the high sugar content found in fruit juices. An 8-ounce serving of juice with sugary fruits such as apple, pineapple or grape can have up to 44 grams of sugar. “Juicing has become a big hit with my patients,” said Priya Massand, a health educator at Montefiore Medical Group on 2300 Westchester Ave. “In an area that is so laden with diabetes it’s almost a dangerous trend because it’s not being done in an educational way.”
Health educator Priya Massand warns patients about juice bars that add agave syrup, honey or enhanced protein powers that are high in sugar. (JENNIFER LUNA/BronxInk)
Massand said she recommends that her patients drink juice that includes only one fruit, not several mixed together, and that they make sure no sweeteners are added. The educator keeps photocopies of the juice bars’ menus and points out which beverages are best—vegetable-based drinks—for her diabetic patients. “It can help but I think it requires so much attention to detail that is being missed that it’s not helping yet,” Massand said. “I’m concerned that it’s a trend and not a lasting change.”
One Monday in October, therapist Shlomit Levy was called to a classroom at I.S. 313, a middle school on Webster Avenue in the Bronx where she has worked for the last four years. A student was causing disruptions, storming out of class.
The clinician from a nearby mental health clinic, Astor at Highbridge, took the student aside for a two-hour therapy session. The student was able to return to class with the help of Levy, but not for long. Half an hour later, she had lost control again.
In her emergency session, Levy discovered the student’s family was not cooperating with her therapy. If Levy had been able to see the child earlier, the crisis might not have happened.
But last year, the state pulled its Clinic Plus funding that required I.S. 313 to have parents fill out mental health assessments for their children. Now that the program is gone, the clinician has no information about which children may need help.
The result is that Levy now in October has only one new student patient, at a time when she usually has at least 10. “I’m missing a lot of information,” she said.
Shlomit Levy, a clinician for Astor at Highbridge in I.S. 313, is seeing far fewer children ever since the clinic lost its state funding. (VALENITNE PASQUESOONE/The Bronx Ink)
Levy’s referral numbers from schools in no way reflects the area’s need. The only mental health outpatient clinic for children and teenagers in the Highbridge section of the Bronx, Astor at Highbridge serves more than 400 clients ages 2 to 21. Patients are seen in its Shakespeare Avenue clinic and inside six local public schools. Its future is uncertain in a community where 52 percent of the population has already received mental health treatment or counseling. In 2006, mental illness hospitalization rates were significantly higher in Highbridge and Morissania than in the rest of the Bronx and New York City.
Levy said the children she sees are suffering from trauma and anxiety among other issues. Some of them have lost a family member to gang violence, or have been sexually abused. Others have parents who are either arrested, incarcerated, or deported. Levy has had patients who lost all contact with their deported parent. Undocumented, these students can’t leave the country to go visit them.
“All these children have such challenging life environments,” Levy said. The therapist is convinced five clinicians like her are needed in I.S. 313. “And we would all be very busy.
The end of Clinic Plus not only curtailed services for needy children, but also created a greater financial problem for the clinic. It came at a time when Astor at Highbridge is being squeezed by yet another cut in state funding. Since 2010, New York State has gradually reduced its direct support for Astor’s two outpatient clinics in the Bronx by 25 percent per year. The same day Levy was called to P.S. 313, the clinic received word that a third 25 percent reduction would go into effect next year, totaling 75 percent lost revenue in three years. The cuts mean clinicians are under pressure to increase the number of clients who bring in Medicaid or private insurance money.
Astor at Highbridge opened the satellite clinics in schools in 2007. The clinic now has six clinicians who work in neighboring schools. Astor was keeping these services afloat after Clinic Plus money ended, yet times are difficult.
“A couple of my schools want more clinicians,” said Zory Wentt, program director at the Astor at Highbridge clinic. “Do we need it? Yes. Are we going to get it? No. We don’t have enough funding for that.”
Wentt has worked a Astor at Highbridge since it opened seven years ago. It remains the only mental health clinic in the area. It was difficult at first to convince residents to overcome their fears and seek therapy, she said. A strong stigma attached to mental health needs was a barrier.
“A lot of children need mental health services. Yet they have never received it,” Wentt said.
A book Levy and other clinicians use to help students in schools. (VALENTINE PASQUESOONE/The Bronx Ink)
At the clinic, therapists see children with conditions ranging from attention deficit-hyperactivity or oppositional defiant disorders to those with bipolar or suicidal symptoms. Violence in the area spills over into their clinic. Trauma and post-traumatic stress disorders are common illnesses.
“We had a little girl whose father was shot right in front of her,” Wentt said. “We have a lot of death cases, along with children being placed in foster care or suffering from sexual trauma.”
In a neighborhood where 35 percent of residents live below the poverty line, according to a study by Queens College, lack of resources can become a triggering factor when it comes to mental illness. The majority of the clinic’s patients are low-income, Hispanic and African-American residents. Eighty-five percent of them are on Medicaid and 5 percent have no insurance. Only 10 percent can afford a private health insurance. Revenue from these insurances is now Astor’s only chance to survive financially.
“Funding is a challenge, we’re constantly out there seeking private funding,” said Sonia Barnes-Moorhead, the executive vice president of the Children’s Foundation of Astor. Astor Services for Children and Families operates 12 sites in the Bronx, including two outpatient clinics. Clinicians have had to provide the same services in a way that could decrease costs.
Astor at Highbridge has been affected by what appears to be a national trend: increasing and larger cuts to mental health state funding.
According to the National Alliance on Mental Illness, more than $1.8 billion has been cut from mental health state budgets in the U.S. from 2009 to 2011. At the same time, one in 10 American children have serious mental health conditions like depression or stress disorder. New York is the second state where cuts are the largest, after California. It cut $204.9 billion in its mental health budget between 2009 and 2012.
Three years ago, the New York State announced it would reduce its Comprehensive Outpatient Program Services (COPS) funding by 25 percent each year, until no funding is left. The state increased Medicaid rates to keep outpatient clinics afloat, but centers like Astor at Highbridge face direct consequences. The COPS funding represented half of the clinic budget, about $1.5 million.
Services at the clinic have been reorganized, and the workload has become barely manageable for some therapists. In 2009, a clinician had about 20 cases in total. Now, their caseloads vary between 50 and 55 people.
“We’ve had to work harder, we’ve instituted a business-like model in mental health services,” Wentt said.
The mental health clinic started to launch open access sessions four days a week for three hours in order to build their client base.
Things can easily become hectic during open access time. Children cry when their parents meet with the therapist, leaving them in the waiting area. Crises can erupt when children fight. A parent advocate and front desk receptionists are available to care for them, but they can often feel overwhelmed.
“With open access, no one is allowed to have a free moment when people come in,” Wentt said.
Zory Wentt has worked at the Astor at Highbridge clinic since 2005. (VALENTINE PASQUESOONE/The Bronx Ink)
With Astor’s limited staff, new clients are often left waiting. On Oct. 1, Nilza Martinez, a 26-year-old resident of Highbridge took advantage of open access hours. She and her 6-year-old child waited for more than an hour, only to be given an appointment two weeks away. No Spanish-speaking clinician was available that Monday.
Her son’s pediatrician at the Bronx-Lebanon Hospital Center had referred her to the Astor clinic. Her son, she said, was showing extreme anxiety about sleeping, and being left alone.
Clinicians said their heavy caseloads prevent them from being entirely available during open access services. Every week, they need to have an average of 25 billable hours of direct contact with their clients to keep the clinic alive. Some of them say they have to schedule appointments almost every hour to maintain this requirement.
“There is a lot of pressure since we have a lot of paperwork and accountability on top of the work you do in sessions with the children and families you’re working with,” said Audrey Williamson, a 26-year-old social work intern working as a full clinician at the clinic since September. She works 21 hours a week at Astor at Highbridge, besides her classes at Columbia University School of Social Work. She is required to see her clients for at least 10 billable hours.
“Yet I think the pressure of helping and assisting children and their families is much bigger,” Williamson said. “You have lives in your hands for the most part.”
On most days, Dagger John’s restaurant at Fordham University earns its reputation as the most popular on-campus eating place. Students gather in the spacious dining area with music playing in the background.
But on Sept. 27, the music disappeared and half of the tables were taken over by baskets of vegetables and food scales. Half a dozen people gathered around each table, checking out and selecting vegetables and there was a line of customers extending out the door.
The interloper is officially called the St. Rose’s Garden Community Supported Agriculture Market. It is a cooperative vegetable buying club that invests in Norwich Meadows Farm in upstate Norwich, N.Y. The founder is Jason Aloisio, 27, an ecology Ph.D. student at Fordham, who is also the founder of an on-campus farm, St. Rose’s Garden.
Aloisio also works at the education center at Prospect Park Zoo, connecting teenagers with nature. (YI DU/The Bronx Ink)
“I love eating good food,” said Aloisio, “and I want people to connect to the nature through food. I want them to put their hands in soil, to see what food look like originally.”
Aloisio sees St. Rose’s Garden and the co-op farmer’s market as ways to help make diets healthier in the Fordham community and even the Bronx at large.
People can buy cheap organic vegetables, including tomato, parsley, radish, soybean, turnip, pepper, carrot and garlic grown in St. Rose’s Garden, or they can join the co-op and receive different fresh vegetables every Thursday from Norwich Meadows.
St. Rose’s Garden is believed to be the only on-campus garden in the Bronx; the only other on-campus farmers’ market is at Albert Einstein College of Medicine.
Growing up in Shoreham on Long Island, Aloisio learned to eat healthy food. As a child, his father, a dentist, kept no candy or desert at home. Fast or processed food was also rare in his home.
“We always had cooked food,” Aloisio said, “so I grew up with real good food.”
Throughout his four years at Fordham, Aloisio has brought that sensibility to the Bronx. When he’s not fulfilling his teaching responsibilities as a Ph.D. candidate, he spends his time on the rooftop of the university parking garage, which he considers his private lab. His dissertation is about “green roofs” in urban areas.
St. Rose’s Garden was originally a piece of unused land that university officials gave to Aloisio to grow edible plants like tomatoes and pumpkins in order to demonstrate new uses for wasted spaces. But he decided instead to use the 1,500-square-foot area to build an on-campus community farm for the whole school.
Aloisio first had this idea of creating a garden on the grounds last year, but wasn’t able to recruit enough volunteers.
This year, Aloisio prepared a formal proposal to change the abandoned land in the unused corner of the school near faculty parking garage into a community garden. He also went to different academic departments, trying to get at least $1,750 to buy essential materials for the garden.
The proposal earned Aloisio a little more than the minimum from three deans at Fordham University who also volunteered in the garden’s construction.
In April, Aloisio and Elizabeth Anderson, an undergraduate student studying environmental policy, started advertising for more volunteers through blogs and by sending emails to students.
On April 23, more than 50 volunteers, including students and faculty members, showed up to assist Aloisio and Anderson building the garden. They removed weeds, built eight raised beds covering 244 square feet and bought 20 cubic yards of soil to fill them. They also laid a water system and planted seeds that blossomed into rows of eggplants, green beans, green and red peppers, cucumbers, lettuce, tomatoes, pumpkins and basil.
St. Rose’s Garden is now producing more than 10 kinds of vegetables. (YI DU/The Bronx Ink)
St. Rose’s Garden offered up its first harvest in September. Green leafy vegetables poked out of their beds. Eggplants turned purple and hid under big leaves. Pumpkins were still in the yellow flower phase, quietly waiting their turn to ripen into fruit.
The garden has also helped grow other efforts at Fordham.
John van Buren, the director of Environmental Policy Program who serves as the faculty advisor for St. Rose’s Garden, is including eight hours of volunteer work at the garden as part of his class.
“Aside from providing fresh, organic vegetables, and an opportunity for playing in the dirt,” said Aloisio, “the underlying mission of St. Rose’s Garden is to be an educational catalyst, both in the classroom and in social settings, for discussion about the broken food system and coupled human-ecosystem interactions.”
He seems to be reaching that goal. “He (Aloisio) is very outgoing, a good person to get things going,” said Joe Hartnett, a junior biology student in the environmental policy class who was one of the volunteers. “He always makes things clear. He is a really good teacher.”
Aloisio was Hartnett’s assistant teacher when he was a freshman. Hartnett said Aloisio brought a lot of different ideas to their environmental classes, making their studies fun and easy to understand. “He is very vocal and energetic,” said Hartnett. “In his email to me, he would say something like ‘Yes, Joe. You CAN do this!’ ”
“He is so passionate,” said Samir Hafez, an economics and environmental policy graduate student. “I admire him for his energies. He never gets discouraged.”
Aloisio says the food co-op is another important component of his campaign to encourage healthy eating.
Consumers pay $16 per week to get a share of six to eight pounds of vegetables and fruit. They agree to buy produce from the farmers for 10 weeks. The vegetables are delivered to Dagger John’s every Thursday for less money than in the supermarket because there is no middleman.
Consumers don’t know what they will get for the week; it depends on what’s available. All the vegetables are picked less than two days before the market.
Katie Buckle, a sophomore at the Gabelli School of Business, did some math with her two roommates. They realized that it would only cost about $5 per person to receive more than enough healthy fruit and vegetables so the three of them decided to pool their money and buy a share together.
“The local farmers send whatever produce they have freshly harvested that week, so our weekly bounty will change and we will likely receive new fruit and vegetables we’ve never tried before,” said Buckle. “To me, this element of surprise is the best part.”
There are currently 137 shares of the co-op, more than Aloisio expected. “We were aiming for 50, and we got 137!” said Aloisio. “I was a little overwhelmed.”
Three resident assistants bought some shares to set up a little farmers’ market in their dorms.
“It helps me to keep a healthier diet,” said Jordan Higgins, a senior biology student. Higgins said she had to Google how to cook much of the produce, but it made her eat more vegetables.
Norwich Meadows Farm also provides vegetables to students at Fordham’s Lincoln Center campus.
Both the co-op and St. Rose’s Garden share space at Dagger John’s. The student-run farmers market allows people who didn’t buy a share in the co-op the opportunity to enjoy fresh vegetables.
John Craven, a Fordham business professor, was one recent satisfied customer. “This is the best baby carrot I have ever had,” he said as he sampled a small fresh carrot grown in St. Rose’s Garden. He did not even scrub off the mud before he ate a second one.
Money earned by selling produce from St. Rose’s Garden goes to the daily maintenance of the garden.
“This is really not for profit,” said Aloisio. “We just want to get the food to people.”
The first day of the two markets was especially long for Aloisio. More than 200 people stopped by. Even though there were three volunteers helping him, Aloisio still had to answer all the questions about the food and the garden, organize containers and refill vegetables, and find bags for those who forgot to bring one.
St. Rose’s Garden has donated a total of more than $1,000 worth of vegetables to Part of the Solution since the first day of the farmer’s market. (YI DU/The Bronx Ink)
Four full containers of vegetables were left after the first day. Aloisio and his volunteers donated all the vegetables to a local non-profit group called Part of the Solution. These vegetables are repacked in Part of the Solution’s food pantry.
Aloisio would like to have more efforts in the Bronx beyond Fordham. Statistics from the Department of Health show that only 6.3 percent of Bronx residents eat the recommended five daily servings of fruit or vegetables.“I hope to get more people involved,” he said, “Maybe refugees in the Bronx can come and work in the garden. Or maybe make it a refugee garden or a asylum garden.”
At the moment, however, it’s hard for people outside of the Fordham community to benefit from the garden. Visitors have to show a valid ID and pass a security guard to get on campus.
In the meantime, Aloisio is focused on keeping St. Rose’s Garden working smoothly.
All volunteers work on a weekly basis now. But as the mid-term approaches, a lot of students are too busy to help. Aloisio dedicates most of his time to the garden.
“I have free time, somewhere, not really,” said Aloisio, as he dropped off four containers of vegetables at Part of the Solution — alone.
Students at P.S. 73 warm up for their health lesson.
At 8:15 am Thursday, nearly 30 4th graders sent mini tremors through P.S. 73.
“Who can last longer than Mr. Rios?” said Juan Ramon Rios, director of Healthy Highbridge. He was trying to get children half his height through a warmup routine of jumping jacks.
Despite all the activity, 37 percent of the students in this class are overweight or obese, according to body mass index measurements that Rios and his team at Highbridge Community Life calculated this week. Two classes even measured in at 59 percent.
The overall rate of overweight students at the Anderson Avenue elementary school is consistent with that of the entire South Bronx, where 40 percent of students are overweight or obese. That percentage is higher than the alarming national level, which the American Heart Associationestimates at 33 percent.
Healthy Highbridge meets with fourth and fifth graders at P.S. 73 once a week to combat the repercussions of obesity in an area that has a lot of obstacles to staying healthy. In the South Bronx, 38 percent of the residents live below the poverty line, according to the 2010 American Community Survey. Highbridge also has too few supermarkets to meet the needs of its 34,000 residents, a 2008 city study says. Rios said these factors lead to poor food choices and, by extension, poor health for area children.
“We’re losing a generation,” Rios said three days earlier from his cramped basement offices at Highbridge Community Life Center. “All of this is going to create a health cost”—that is, unless everyone gets moving.
After the exercise, Rios instructed students on how to take their pulses.
“Why did we do that?” Rios asked as 60 index and middle fingers pressed against 30 wrists.
“To lose some weight,” said Fatumata, 9.
“Because it could be fun to exercise,” said Shantel, also 9.
“Because we need to get exercise,” said 10-year-old Jonah.
These children are all participants in Healthy Highbridge’s year-long health education program, funded by a $30,000 grant from the Communities Impact Diabetes Center, which in turn receives its budget from the federal Centers for Disease Control and Prevention.
Before they start their education curriculum, Healthy Highbridge staff must measure the students’ body mass indexes, test their prior health knowledge and survey them on exercise and eating habits as well as their attitudes and beliefs regarding working out and eating. These initial studies will be used as a baseline to track students’ progress, as Rios and team return each week to tackle a different health subject: Michelle Obama’s “My Plate” and “Let’s Move” campaigns, diabetes, nutrition, and exercise, among others.
P.S. 73 students eat a breakfast of sausage, biscuits and orange juice.
The goal is to help youngsters understand what it takes to be healthy, said Michelle Ramos, the diabetes center’s community project manager.
“As attitudes around healthy behavior improve, hopefully the behavior itself will improve,” she said from her Harlem office. Ramos said that while she doesn’t encourage children to lose weight, she believes that as they grow, they’ll maintain their weights and their body mass indexes will drop.
“Hopefully they’ll pick up healthy habits and go and share them with their families,” Ramos said.
P.S. 73’s principal, Jean Mirvil, said sharing health information with the parents is critical to solving the obesity problem. Many of the families, he said, come from different countries and have a hard time making the proper, healthful adjustments in their new homes (34 percent of people in the South Bronx are foreign-born).
“The kind of food they’re used to does not present itself in the same way as they are making the adjustment with this country,” Mirvil said.
He expects that the children will bring information about what and what not to eat home to their parents.
“At school, they are given a full picture of what a regular, healthy meal should look like,” Mervil said.
To combat the obesity problem, this September the school instituted a salad bar at lunch, so students can add a rotating variety of produce—spinach, corn, radish—to their meals. The main courses vary according to the Board of Education menu. Recently, Mervil said, students had chicken and a choice of pasta or rice. Students can choose milk—not chocolate milk—or water for a beverage.
On the day of the Healthy Highbridge visit, breakfast consisted of a sausage and biscuit sandwich, and orange juice.
During this class, students were asked to pick which food choices they would make: chicken with the skin on or off, whole wheat or sweet bread, regular peanut butter or freshly ground.
Shannon takes her pulse after a round of jumping jacks.
Shannon, 9, said she preferred popcorn without butter, low-fat milk to skim, and would eat an apple before a piece of candy most days.
“Salt? Ew,” she said, her neat cornrows jostled back as she shook her head.
Winston, the largest boy in the class and the first to cease his jumping jacks, said he was less into self denial. He puts butter on his popcorn because, otherwise, “it doesn’t taste like anything.” The nine-year-old did acknowledge that salt isn’t always necessary.
“Sometimes, if you don’t add salt, food can still taste good,” he said.
Jaheim, 10, said he couldn’t replace french fries with potatoes, nor could he exchange a burger for a salad. “French fries?” he asked rhetorically as his hands shot from his striped hoodie to the sky. “I love them.”
As for burgers? “They’re very good,” he said. “You could even put bacon on them.”
When asked if all his poor eating choices left him a healthy individual, Jaheim was confident.